CONTINUING MEDICAL EDUCATION
NeuroSurgery Training
NeuroSurgery Training by Dr. Cherian
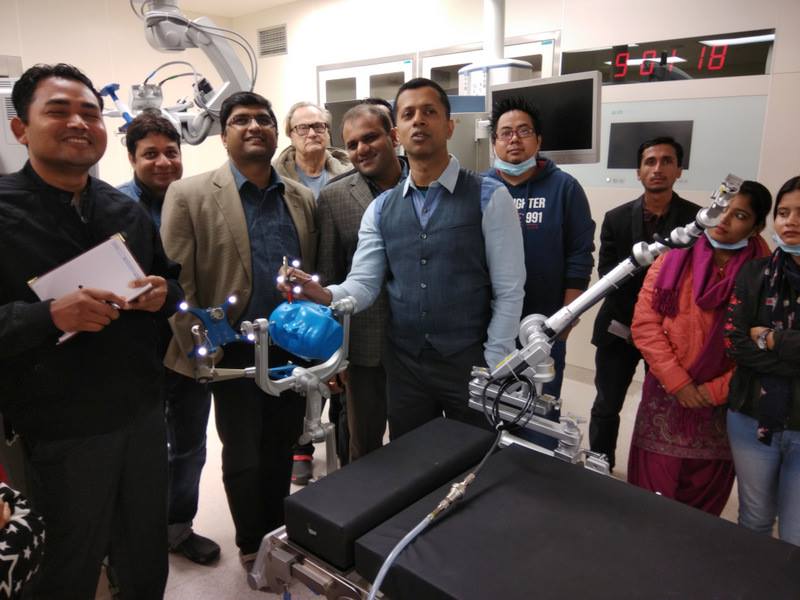



Neurosurgical training at Krishna Institute of Medical Sciences, India for fellows and residents with excellent facilities will soon be announced.
Neurosurgery Fellowship Programme at the Institute of Neuroscience, Krishna Institute of Medical Sciences, Karad, India
The training is meant for residents, young neurosurgeons and mid-level neurosurgeons who would like to improve their knowledge, skills and strategies in skullbase, vascular and endoscopy. The training involves cadaveric dissections, micro-vascular anastomoses, watching surgical videos, assisting surgeries, discussing strategies, complication management and many more areas which would improve surgical skills and attitudes for excellence in neurosurgery.
More details and signing up for the fellowship programme will be announced shortly.
NEUROSURGERY
Cisternostomy
Cisternostomy is a micro-neurosurgical procedure to drain the cerebrospinal fluid from the basal cisterns in order to reduce the intracranial pressures arising from the CSF shift edema in the setting of moderate to severe brain trauma. It was invented by Dr. Iype Cherian over a decade ago. after it appeared to him that opening the membrane of liliequest in a traumatic brain played a positive role in rapidly decreasing the intracranial pressure (ICP) and also resulted in a better prognosis. The initial years of research and modified surgical procedures along with a combination of decompression coupled with cisternal drainage opened up roads to advances in surgical management of brain trauma. Additionally, the studies on the glymphatic system indicating a clear communication of the CSF with brain parenchyma validates the physiological basis of cisternostomy as a more effective alternative for reversing CSF shift than traditional procedures like decompressive hemicraniectomy, whose basis is the primitive practice of trepanation, and which more often than not results in severe and irreversible axonal damage due to unavoidable brain swelling the procedure entails.
The recent years have seen a trend in both worldwide acceptance and some reluctance to adopt cisternostomy as protocol for management of brain trauma. However, the vastly improved outcomes and evident prognoses in many centres around the world have created waves in neurotraumatology. The on-going neurotrauma study, Global Neurotrauma Outcomes Study funded by the NIHR regards cisternostomy as one of the choices to reduce ICP in emergency traumatic brain injury (TBI). With ongoing studies and training opportunities for young neurosurgeons to skillfully perform cisternostomy, it has been steadily revolutionizing the current management of traumatic brain injury while also being adapted for treatment of various other conditions.
Technique
Cisternostomy is performed utilizing an anterolateral skull base approach with a fronto-temporal craniotomy following a keyhole on the zygomatic arch. A layer-by-layer dissection allows for a fine reconstruction upon closure.
Extra-dural maneuvers to “unlock” the brain allow for unfolding of the brain folds at the fronto-temporal junction, in the sagittal and axial planes.
Unfolding in the sagittal plane involves the removal of as much sphenoid bone as possible, followed by a sharp dissection of the Orbito-meningeal band that unlocks the brain in the axial plane. This ultimately flattens out the convexities of the brain allowing more space for the edematous brain to lax in moderate to severe traumatic brain injury. A transcavernous peeling of the temporal dura from the cavernous sinus while preserving the True Cavernous Membrane (TCM). This modification maintains the integrity of the nerves in the cavernous sinuses and prevents bleeding that otherwise occurs in a Dolenc’s approach.
Additional maneuvers to obtain a wider access to the inter-optic cisterns involves the removal of the anterior clinoid process that is visible after OM dissection. The OMB, which connects the orbit to the frontal and temporal dural layers and covers the anterior clinoid process.
A basal dural opening is then made and the subdural hematoma evacuated. The laxity achieved through extradural unlocking maneuvers enables one to reach the interoptic cisterns with minimal retraction and/or ACP removal.
The intra dural carotid (C2) and the optic nerve can be visualized and the membrane of Liliequest is cut through the optico-carotid window to open the basal cistern. A number 8 feeding tube is inserted to drain the CSF from the cisterns. One can instantly observe a rapid decrease in brain tension and a regain of pulsatality in the brain matter. The dura is closed with approximation and the drain is left in place for at least 5 days for continued CSF drainage that helps prevent the cascade of secondary damage, by efficiently regaining the CSF flow and enabling the cooling and cleaning of the brain from metabolic heat and wastes respectively.
Quick Facts
- Almost 10 million people affected annually worldwide.
- 106 persons in every 100, 000
- As high as 150 – 170 in Africa, and some parts of Asia and Latin America
- Mortality rates 6 times higher in low and middle income families
- Decompressive hemicraniectomy (DHC/DC) for TBI management results in 34.8% mortality
- Cisternostomy for TBI management has less than half the mortality rate of DHC/DC at 13.8%
- DHC/DC requires on an average 6.3 days on Ventilator
- Cisternostomy requires 2.4 days on an average on Ventilator
- DHC/DC requires on an average of 19.4 days in ICU
- Cisternostomy requires patients to be in ICU for only an average of 4.4 days
CSF Shift Edema
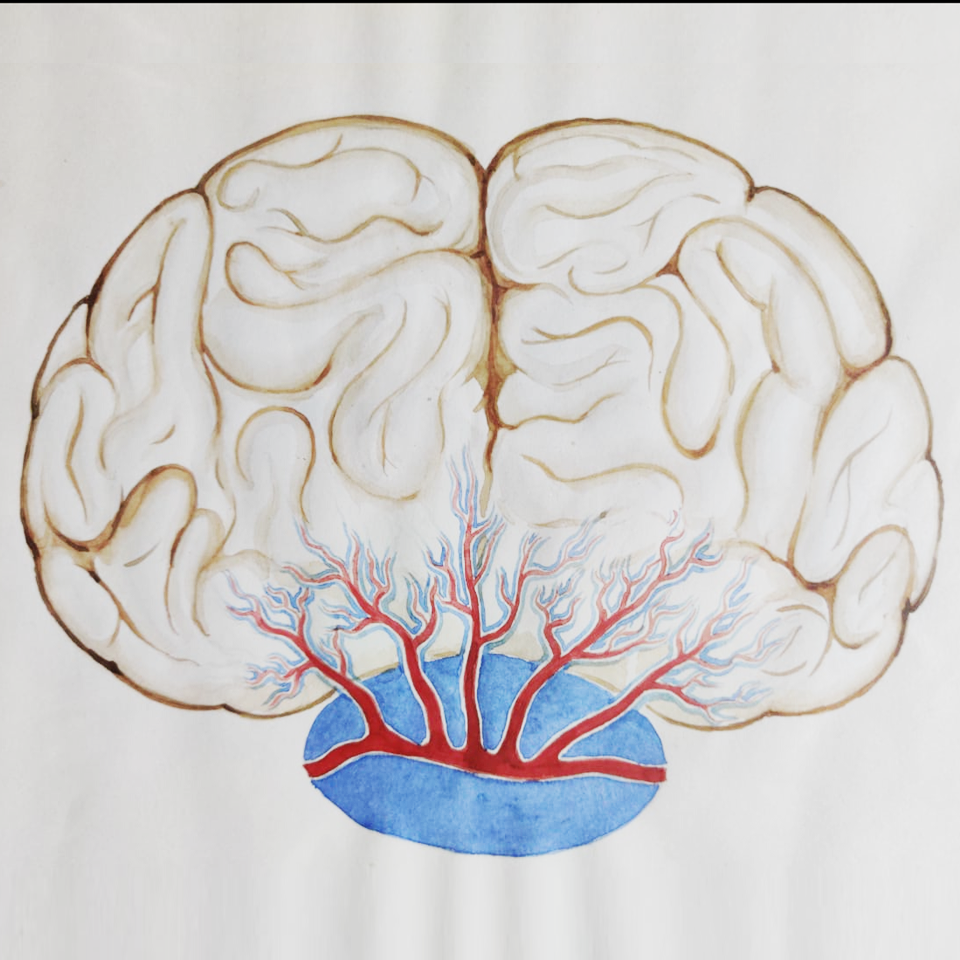
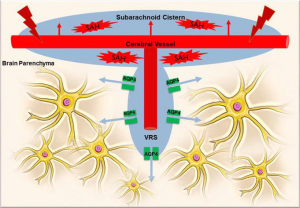
CSF shift edema is defined as the mechanism by which the CSF enters the cerebral ISF as a result of the shift of CSF from the subarachnoid cisterns into cerebral parenchyma following hemorrhage within the sub-arachnoid space. The rising pressure within the subarachnoid space forcing the CSF into the brain parenchyma via the Virchow Robin Spaces, giving a picture of classic cerebral edema and features of raised intracranial pressure.
Pathophysiology
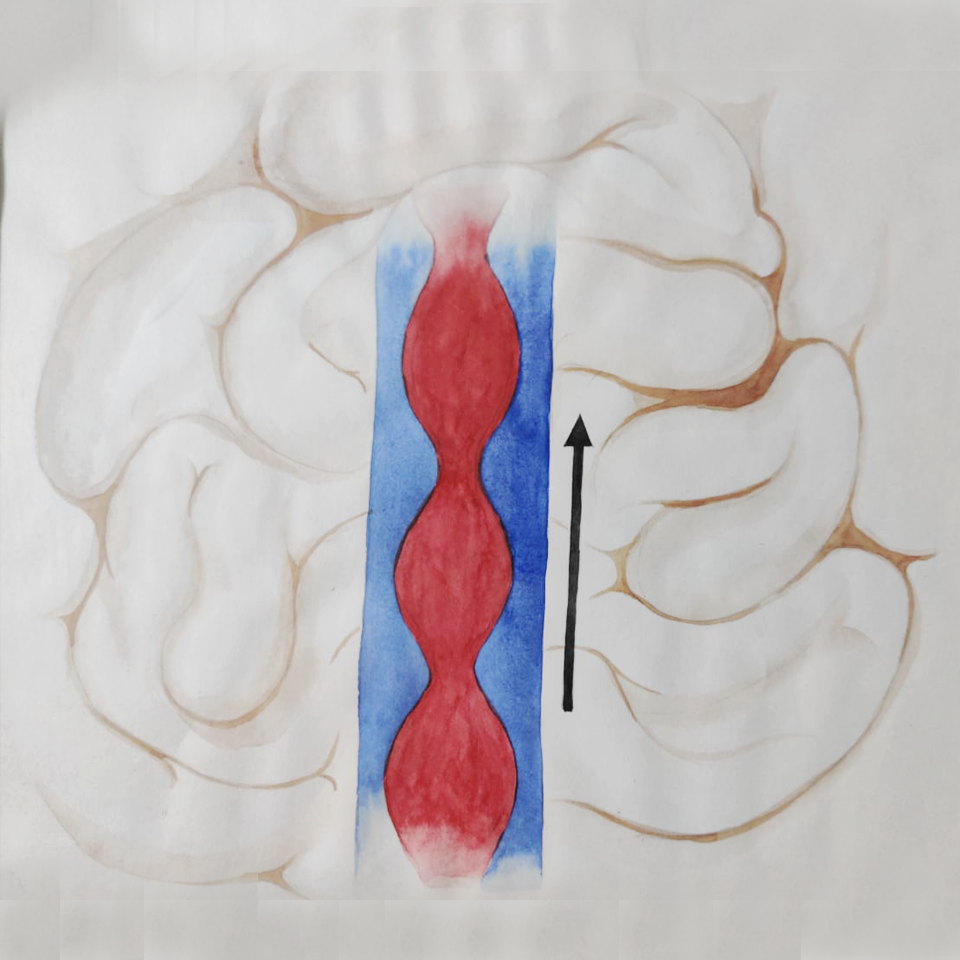
The cerebral arteries are bathed by the sub-arachnoid spaces and penetrate the brain parenchyma providing a rich blood supply. These vessels are accompanied by a surrounding para-vascular, or more precisely, the Virchow-Robin Spaces, that are extensions of the sub-arachnoid cisterns containing a high volume of circulating CSF. Lining these VRS, the endothelium acts as a barrier between the ISF and the cisternal CSF, gated by the aquaporin channels. In setting of SAH, the leakage of cerebral vessels occupies the cisternal spaces with blood, increasing cisternal pressures due to hydrostatic forces which push out the CSF through the VRS endothelium into the brain parenchyma. Depending upon the severity of the insult to the cerebral vessel, the amount of hemorrhage determines the shift of the CSF out of the cisterns that ultimately leads to a complete obliteration of the basal cisterns as seen in a radiological image of a herniating edematous brain.
NEUROSCIENCE
Cleaning and Cooling Theory

Cleaning and Cooling Theory is a hypothesis developed by Dr. Iype Cherian. It argues that cerebrospinal fluid (CSF) has properties and functions that go beyond the traditional understanding and assumptions about its role in the nervous system and that its regulatory importance has been previously overlooked. The theory was developed from observations of the outcomes and prognoses of cisternostomy, a neurosurgical procedure, invented by Dr. Cherian for them management of traumatic brain, and the recent discovery of the brain’s glymphatic system.
Cleaning and cooling theory puts forward the idea that besides the previously established functions of CSF, thought to be for cushioning and providing buoyancy to the brain and central nervous system, it also has a very crucial role in removing interstitial waste particles of the brain while maintaining its temperature. The glymphatic circulation of CSF to and from the brain via ventricular and, more adeptly, paravascular pathways are theorized to be for the purpose of “cleaning” the brain while the close proximity of the basal cisterns to the sinuses and their effect on the CSF circulation is assumed to be for the purpose of “cooling” the brain.
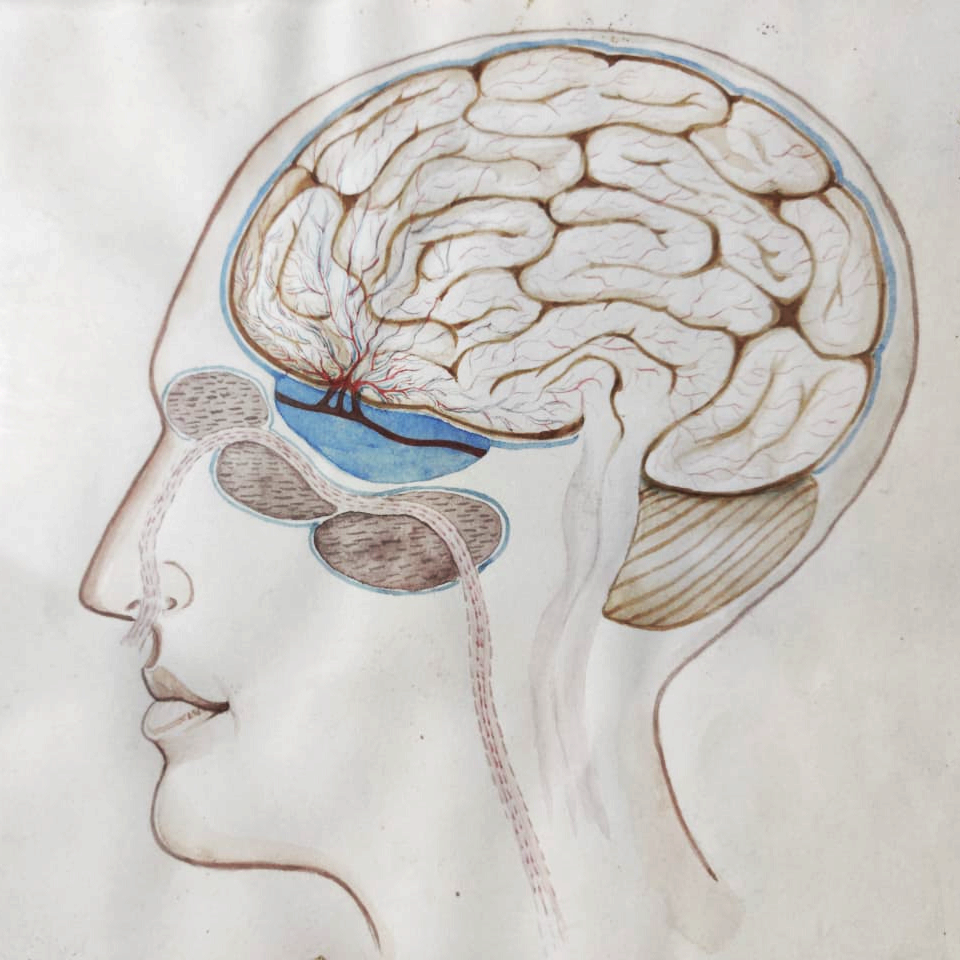
Studies have shown that a decrease in temperature can assist in reducing brain swelling and this fact has also sometimes been used to manage the traumatic brain. The fact that the portion of the face around the sinuses have lower temperatures when compared to the rest of the face led Dr. Cherian to conjecture that the close proximity of the sinuses to the basal cisterns is for the purpose of controlling the temperature of the brain by cooling the CSF that passes through it. This led him to believe that the moisture produced by the seromucous glands act in tandem with the airflow from the turbinates and causes the temperature of the surrounding areas to drop. The direct consequence of this is the cooling effect it has on the basal cisterns, which are surrounded by the frontal, sphenoid and ethmoid sinuses. Because of this, “cooled” CSF enters the brain from the cisterns and encourage healthy parenchymal activity.
Dr. Cherian explains that the effect of the moisture and airflow in the sinuses is somewhat analogous to the effect lines of wet clothes would have in a well-ventilated room’s overall temperature. Similarly, knowing that CSF reabsorption into the systemic circulation occurs via the venous system at the arachnoid granulations in the superior sagittal sinus, it can be surmised that it is bound to be affected by the sinuses.
At the same time, the active production of CSF at the rate of 500 ml. a day means that the role of the fluid is also the removal of interstitial dirt such as tau and beta protein that are generated by the biochemical reactions taking place in an active brain. The discovery of the glymphatic system suggested that CSF allows movement of metabolites, toxins, and nutrients, and has a role in homeostatic hormonal and signalling mechanisms, chemical buffering and neurodevelopment. All these facts have helped justify Dr. Cherian’s assumption about the interstitial waste removal “cleaning” function of the CSF, and it is the CSF-ISF exchange that drives the removal of exogenous and waste molecules from the interstitial spaces of the brain.
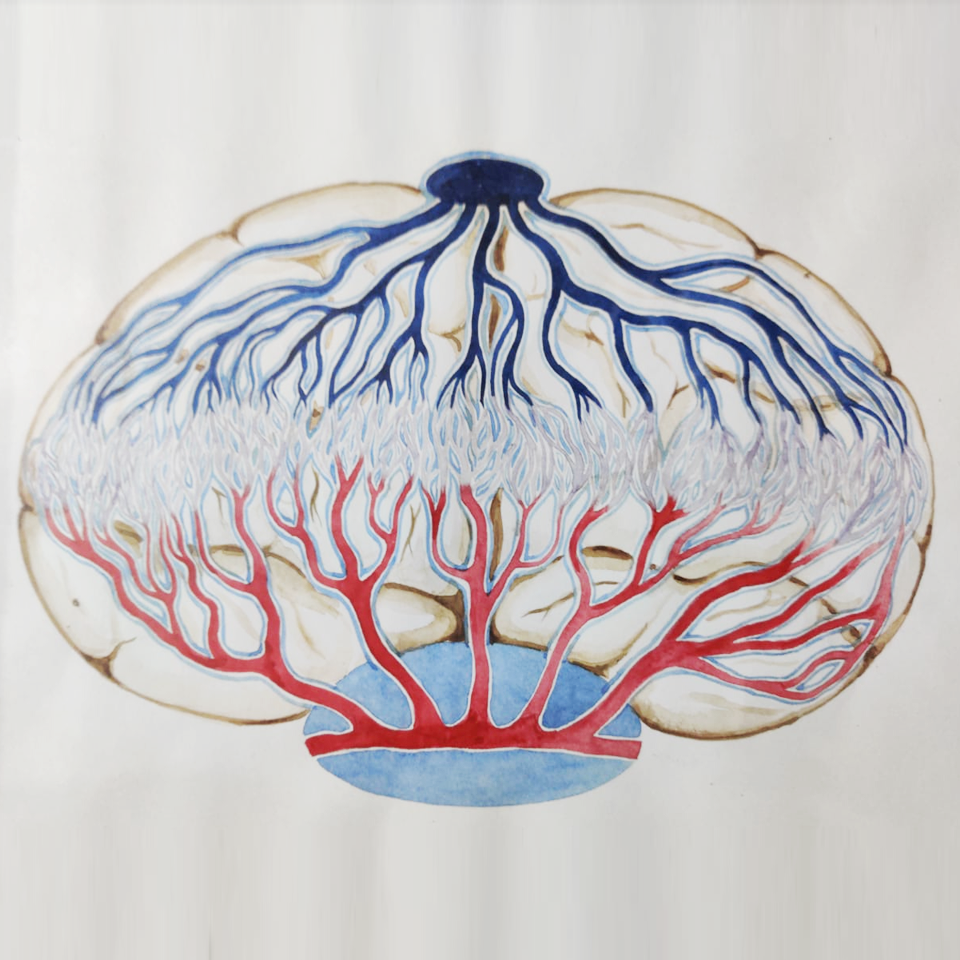
The difference in hydrostatic and osmotic pressure between the arteries and veins under normal physiological conditions transports water and molecules in a way that while water enters from the arterial side, molecules enter from the venous side along with soluble wastes. This explains why the reabsorption of metabolic waste occurs in the venous side (paravenular efflux). The movement of the fluid literally acts as a cleaning shower for the brain. This might explain why the brain is the only organ in the human body in which the main arteries and veins do not run parallel but is in totally opposite directions.
Additionally, his theory also puts forward the proposition that normal breathing also has a potential role and formidable impact on the clearing and cooling mechanism of the brain as it increases the movement of fluids through the brain and thus improves the flow of molecules, as well as bringing down the temperature of organ as a whole.
Read
“A Unified Physical Theory for CSF Circulation, Cooling and Cleaning of the Brain, Sleep, and Head Injuries in Degenerative Cognitive Disorders”
Chapter from the book authored by Iype Cherian and Margarita Beltran
Abstract: Cerebrospinal fluid (CSF) from the basal cisterns transits into the brain through spaces that surround the vascular system of the brain; the so-called paravascular spaces (Virchow Robin Spaces), or paravascular pathway, which surround the arteries, veins, and capillaries. The passage of CSF through these paravascular spaces is driven by the cardiovascular and respiratory systems, and is more active at night during sleep. Their cumulative function is presumed to include the clearance (or “cleaning”) of metabolic wastes, which likely contributes to counteracting metabolic heat, via the “cooling” of the brain. This paravascular CSF transport system might be implicated in CSF shift edema that occurs in head injuries; hence, it may be the rationale behind why opening the cisterns to atmospheric pressure through cisternostomy, quickly decreases post-traumatic brain swelling. When this paravascular system is blocked or becomes somehow dysfunctional, the “cleaning” and “cooling” functions of this system may be impaired or completely stopped. This could result in the accumulation of metabolic wastes that cannot be removed within these spaces. In addition, a faulty brain cooling system might play a role in the modification of the molecular structures of proteins, thereby making them more difficult to be removed by the flow of CSF, thus aggravating the situation. Therefore, this may be a common underlying mechanism for many neurodegenerative disorders, and an aggravation factor for others. This avenue appears to be novel and promising toward the elucidation and treatment of a host of diseases.
Brain Cooling and Cleaning: A New Perspective in Cerebrospinal Fluid (CSF) Dynamics
Chapter by Hira Burhan and Iype Cherian from the book Cerebrovascular Diseases (Working Title) edited by Dr. Patricia Bozzetto Ambrosi, Dr. Rufai Ahmad, Mr. Auwal Abdullahi and Prof. Amit Agrawal, INTECHOPEN
Abstract: The function of the cerebrospinal fluid (CSF) has long been considered for mechanical protection and recently attributed to the supply of nutrients to the brain. However, we hypothesize that the brain is a water-cooled and water-cleaned system. Recent studies on the glymphatic pathways and the introduction of cisternostomy as a surgical procedure for traumatic brain injury reveal a vast and in-depth functionality of the CSF, which works in synchrony with the cardiopulmonary rhythms to act as a buffer for optimum cerebral function. The nasal sinuses are located around the suprasellar cistern, and the evaporating wet mucosa within them during the breathing contributes to local cooling, whereas the nocturnal activation of AQP4 channels allows CSF-ISF exchange. The resultant “cooling and cleaning” of the brain not only maintains a physiological equilibrium but also opens doors for understanding and treating pathophysiology underlying common degenerative and neuro-inflammatory diseases. This chapter describes the novel theory of brain cooling and cleaning and the clinical and experimental evidence to support this hypothesis.
AFFILIATIONS